Direct Anterior Approach for Total Hip Replacement
Omaha Anterior Hip Approach Information by Dr. Ajoy Jana MD
Introduction
When hip pain and stiffness limits your daily activities, and medications and lifestyle modifications fail to provide adequate relief, you and your orthopedic surgeon may decide on a total hip replacement. Total hip replacement has transformed the lives of many people by enabling their return to an active lifestyle with reduced or no pain.
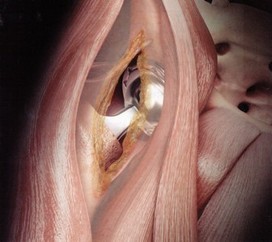
Since 2007, Dr. Jana has been using an innovative technique for doing hip replacements called the direct anterior approach. With this technique, a person can have his or her hip replaced without cutting through muscle or tendon. As you would expect, there are numerous benefits to replacing a hip without cutting muscle. Currently, most orthopedic surgeons perform hip replacement using a posterior or lateral approach. Both of those methods require the detachment of muscle and tendon from the femur. In contrast, the direct anterior approach goes in between muscles in the front of the hip without cutting them. By preserving the muscles and working in between them, patients can recover faster after surgery with fewer restrictions and less fear.
Even though the direct anterior approach was first developed decades ago in Europe, recent refinements to the technique have made it easier to perform. Currently, there are a limited number of orthopedic surgeons trained in this technique. Many people first learned about the anterior approach when golfer Tom Watson came in second place in the 2009 British Open - only eight months after having his hip replacement done through the direct anterior approach. Since Dr. Jana switched to the direct anterior approach, the feedback from patients, therapists and nurses has been tremendously positive.
When hip pain and stiffness limits your daily activities, and medications and lifestyle modifications fail to provide adequate relief, you and your orthopedic surgeon may decide on a total hip replacement. Total hip replacement has transformed the lives of many people by enabling their return to an active lifestyle with reduced or no pain.
Since 2007, Dr. Jana has been using an innovative technique for doing hip replacements called the direct anterior approach. With this technique, a person can have his or her hip replaced without cutting through muscle or tendon. As you would expect, there are numerous benefits to replacing a hip without cutting muscle. Currently, most orthopedic surgeons perform hip replacement using a posterior or lateral approach. Both of those methods require the detachment of muscle and tendon from the femur. In contrast, the direct anterior approach goes in between muscles in the front of the hip without cutting them. By preserving the muscles and working in between them, patients can recover faster after surgery with fewer restrictions and less fear.
Even though the direct anterior approach was first developed decades ago in Europe, recent refinements to the technique have made it easier to perform. Currently, there are a limited number of orthopedic surgeons trained in this technique. Many people first learned about the anterior approach when golfer Tom Watson came in second place in the 2009 British Open - only eight months after having his hip replacement done through the direct anterior approach. Since Dr. Jana switched to the direct anterior approach, the feedback from patients, therapists and nurses has been tremendously positive.
|
What are the advantages of the direct anterior approach?
|
Total Hip Implanted Through the Direct Anterior Approach
|
Animation of Anterior Approach Hip Replacement |
Close-up of a Total Hip Prosthesis  |
Are there disadvantages of the direct anterior approach?
There are a few potential disadvantages of the direct anterior approach that all patients should be aware of:
Although the majority of cases done with the anterior approach do not take any longer than with a traditional approach, there are certain difficult cases that do take more time. Because the anterior approach does not detach any muscles from the hip, the working space is smaller and most surgeons would agree that this makes the surgery technically more difficult than traditional techniques. After having performed hundreds of hip replacements using the anterior approach, Dr. Jana has found that most cases do not take any longer than traditional approaches.
With the anterior approach, there is a greater chance of having numbness around the incision or on the side of the thigh, when compared to a hip replacement with a posterior incision. This is because the skin on the front of the thigh, near the incision, has more nerve branches than the skin on the side and back of the hip. With other techniques, the surgical incision angles towards the buttock - an area with fewer nerves. Most cases of skin numbness improve or resolve over time, but in some cases the numbness is permanent. There is no muscle weakness involved.
Occasionally there is more bleeding during surgery with the anterior approach. This is not a common problem. Dr. Jana uses a "cell saver" during surgery which captures most of a patients shed blood and then allows it to be given back during or after the surgery. It is exceptionally rare that a patient will need a blood transfusion after surgery.
There are certain circumstances where the anterior approach is not the best choice for hip replacement - revision surgeries, severe bone damage, and morbid obesity are examples. About 95% of patients are good candidates for the direct anterior approach.
Why hasn't every orthopedic surgeon switched to this technique?
Here are some possible reasons:
- It is a relatively new technique and many surgeons are not yet convinced it is superior.
- It is technically more difficult and until the surgeon gains enough experience, the surgeries can take longer.
- It takes time and commitment and advanced training in order to develop the skills to perform this operation well.
Is the prosthesis any different with the anterior approach?
With the direct anterior approach, almost any standard prosthesis can be used. That said, most of the implant companies have designed new femoral implants with features that make them easier to insert with the anterior approach. The changes made to the implants are subtle, but very helpful to the surgeon - the femoral stems are a little shorter and more rounded at the top and bottom. No changes were made to the ball or socket parts of the prosthesis.
There are four parts to a hip replacement:
- the femoral stem, which is inserted into your thigh bone and is usually made of titanium
- the ball, which attaches to the femoral stem which is made of either metal or ceramic
- the socket, which is also made of titanium
- the plastic liner which snaps into the titanium socket
What is the usual recovery and follow-up care?
The hospital stay after the direct anterior approach hip replacment averages 1-3 days. The first follow-up visit in the office is 2 weeks after surgery. Some older patients and those who live alone often choose to go to a rehab center for 1-2 weeks. Patients start to walk the day of surgery or the day after using a walker or crutches for assistance. Physical and occupational therapy will take place in the hospital but are not usually required after hospital discharge. There are no restrictions on body or leg positioning - patients are allowed to bear full weight, use a standard-height toilet, cross their legs, and sit in standard furniture including recliners.
Either absorbable sutures or staples are used to close the skin incision. We prefer to use sutures that are invisible and placed below the skin, but sometimes the skin is too thin for this so staples are chosen. A waterproof dressing is used that allows most patients to shower 1-2 days after surgery. Tub baths and swimming are usually restricted for 3-4 weeks.
Patients are encouraged to exercise daily and may gradually return to activities as tolerated. The decision on when to return to work is individualized based on each patient's recovery and the demands of his or her job. It may be as early as 2 weeks after surgery or as late a 3 months. Driving is allowed when the patient is not on narcotic pain medication. Patients are encouraged to wean off of the pain medications a soon as tolerated.
Risks
Every surgery involves some risks and any hip replacement should be considered major surgery. The decision to have surgery should only be made after careful consideration of the risks involved. While uncommon, there are problems that can arise with any hip replacement procedure. The major risks associated with the procedure include, but are not limited to: infection, blood clots, nerve or blood vessel injury, fracture, dislocation, leg length inequality, implant loosening, bleeding, and continued limp or pain. Some of these problems may need further corrective surgery. Not every complication can be corrected and not every patient is satisfied with the results of surgery.
Connect with me on Google +
