Omaha Total Hip Replacement - FAQ
Total Hip Replacement Information by Dr. Ajoy Jana MD
Dr. Ajoy Jana - is a top rated, Omaha Total Hip Replacement doctor, that specializes in orthopedic care. Dr. Ajoy Jana provides total hip replacement surgery to patients in the Omaha Nebraska area at Methodist Physicians Clinic Orthopedics.
Should I have a Hip Replacement?
If the pain and stiffness of hip arthritis interferes with your ability to work, enjoy recreational activities, or perform your usual activities of daily living, then hip replacement may be an option for you. Sometimes people make the mistake of believing that they should be nearly incapacitated before having surgery, but the symptoms do not need to be that severe. Of course, hip replacement surgery should not be taken lightly and it’s important to first try the non-surgical treatment options. Your orthopedic surgeon can help you make an informed decision.
What if I put off Hip Replacement Surgery?
For the majority of people, putting off surgery will not harm the hip in any way. That said, there are occasional cases when the hip arthritis is severe enough to recommend having surgery sooner, so as to prevent further bone damage.
What exactly is being replaced in a Hip Replacement?
The hip joint is a ball-and-socket joint. The head of the femur is the ball and it fits into the part of the pelvic bone called the acetabulum, which is the socket, see Figure 1. During hip replacement, the head of the femur is removed and replaced with a prosthetic ball, which is attached to a stem. This stem is inserted into the hollow canal of the femur bone. A metal cup is fit tightly into the acetabulum. Finally, a liner is placed into the metal cup to take the place of cartilage. Figure 2 shows a hip prosthesis overlaid on an X-ray of the hip.
Figure 1. Normal Hip Anatomy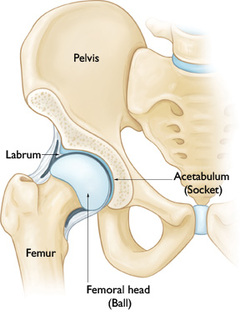 |
Figure 2. Total Hip Prosthesis (overlayed on an X-ray) |
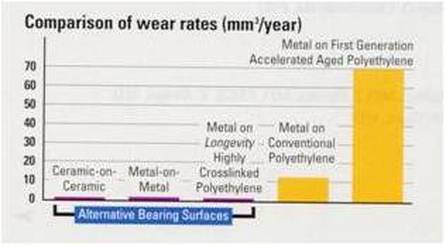
Lots of factors affect how long a hip replacement will last, but the most important one is a person's activity level. The more active you are, the faster your hip prosthesis will wear out, see Figure 3. Other important factors include: age, weight and the type of prosthesis.
Because of technological advances, hip replacements last significantly longer than in the past. Even before the latest innovations, hip replacement lasted 15 – 20 years. Now, they are expected to last even longer. In laboratory testing, the current generation of hip replacements appear to last for decades. Of course, it will take another decade or two to confirm the laboratory results.
What happens if my hip replacement eventually wears out?
If only the plastic liner in the cup wears out, the liner can be replaced while leaving the rest of the prosthesis in place. If the femoral stem or acetabular cup becomes loose, then those parts would need to be replaced also. Of course, replacing all the components is a more involved procedure.
Are there any major breakthroughs in hip replacement on the horizon?
Right now, most research is focused on trying to minimize the amount of wear that takes place between the prosthetic ball and socket. Currently, manufacturers are using a process known as cross-linking to increase the durability of the plastic liner. In simulator testing, the use of this technique has been shown to decrease wear 85% to 95%. Currently, hip replacements are also available that use a metal ball with a polished metal socket, or a ceramic ball with a ceramic socket. These “hard-on-hard” bearings are being closely evaluated to see if they will be any more durable than cross-linked polyethylene. Unfortunately, some problems with these alternative designs have shown up recently.
What are the possible complications and risks of surgery?
All major surgery has some risk of complications. Most problems that occur are correctable, but some can be quite serious or even life threatening. The following list is not intended to cover all of the possible complications related to hip replacement, but to make you aware of some of the more common ones, as well as the most serious.
- Death is a very rare complication but it should still always be discussed. As with any major surgery, death can occur from such things as heart attack, stroke, pneumonia or anesthetic reaction.
- Infection: The chance of getting a deep infection around the prosthesis following total hip replacement is approximately 0.5%. Although the risk is small, infection following joint replacement surgery can be a particularly serious complication - often requiring intensive antibiotic treatment and additional surgery. Some infections may show up very early, before even leaving the hospital, while others may not become apparent for months, or even years after an operation. It is important to know that infection can spread to an artificial hip from any part of the body that has infection. That’s why it is so important to make sure any infection in your body is treated urgently. That is also why it is recommended that people who have an artificial joint take a prophylactic antibiotic before having dental work or any surgical procedure with a risk of bacterial contamination.
- Blood clots (deep vein thromboses or DVT) can form in the large veins of the leg after hip replacement. This may cause the leg to swell, become warm to the touch and painful. A blood clot in the lungs is called a pulmonary embolism (PE) and it can come from a clot that starts in the legs or it can form in the lungs directly. A PE can be very serious and even cause death. One of the most effective ways to reduce the risk of DVT and PE is to get out of bed and start moving soon after surgery. In addition, patients are placed on a blood thinner for 2-4 weeks after surgery.
- Leg length discrepancy: After hip replacement, patients can occasionally feel that the operated leg is slightly longer than the other leg. Leg length measurements are routinely taken during surgery to try to prevent this from happening, but it is sometimes necessary to lengthen the leg in order to maximize the stability of the hip and reduce the likelihood of dislocation.
- Hip dislocation occurs when the hip ball comes out of the socket. This can happen shortly after surgery or many years later. One of the main benefits of the direct anterior hip approach is the low risk of dislocation. With this approach, the risk of dislocation is about 0.5%. The risk of dislocation increases greatly when hip replacements need to be revised. Revision surgeries have a dislocation rate as high as 15%.
- Injuries to nerves or blood vessels are very rare, but can occur during surgery because these delicate structures sit very near the hip joint. Most patients do have some numbness around the incision area but it typically decreases over time. With the anterior approach, the risk of some residual numbness of the thigh is higher because the incision is closer to branches of the femoral nerve than with other surgical approaches. Nerve injuries that effect muscle strength are uncommon and usually resolve as well. Unfortunately, there are rare cases where the damage can be permanent.
- A mild limp may persist, even after fully recovering from the surgery. The limp is usually painless and results from hip muscle weakness. The direct anterior hip approach minimizes this risk.
- Persistent pain despite an otherwise successful surgery is unusual, but can happen. In some cases, pain in the hip area can be a consequence of low back arthritis or other problems. Although many patients do end up with a pain-free hip, it is important for patients to understand that it is normal to have some mild aches and pains after hip replacement. Studies have shown that activity-related thigh pain can develop in up to 3% of patients who have undergone hip replacement surgery. In most instances, the mild to moderate pain can be successfully managed with over-the-counter pain medication.
- Fracture of the femur or pelvis can occur during surgery. In most cases, the fracture can be recognized and fixed immediately without affecting the final result of the operation.
- Post-operative confusion and memory loss can result from narcotic pain medication and anesthesia especially in older patients. Understandably, families are often caught off-guard when this happens and it can be quite upsetting to witness. When it occurs, it usually lasts two or three days.
Do I need to donate blood for myself prior to surgery?
I do not recommend self-donation of blood. Most patients with a normal blood count before surgery will not need a transfusion after surgery, but blood loss during surgery can vary a lot from patient to patient. To minimize the chance of needing a transfusion, I use “cell saver” during surgery that recycles much of the blood that would normally be lost.
If a person would like to donate blood for him or herself prior to surgery, then those arrangements can be made. The reality is that the patients who have a blood count high enough to donate for themselves are the ones who are least likely to need it. Family or friends can also donate for you, but studies have found this not any safer than using blood from the Blood Bank. If your blood count is low (Hemoglobin 10-13 mg/dL) prior to surgery, I will make a referral to the Methodist Blood Conservation Program. When appropriate, intravenous iron and/or a medicine called ProcritÒ can be given to boost your blood count.
How long does hip replacement surgery take?
It takes approximately 1 1/2 - 2 hours for an uncomplicated first-time hip replacement. Some cases take longer depending on a patient’s size, weight, and severity of arthritis. Methodist Hospital provides a nurse liaison to communicate with families and update them during the surgical case, as needed. Keep in mind that the surgery actually starts about 30 minutes from when the patient leaves the pre-operative holding area.
What type of anesthesia is used?
Hip replacement surgery can be done with either general anesthesia or spinal anesthesia. On the day of surgery, the anesthesiologist can help you decide which choice is best for you. Dr. Jana prefers spinal anesthesia for his patients whenever possible because it has been shown in studies to have several benefits over general anesthesia. The benefits include a lower the risk of blood clots, heart attacks, pneumonia, nausea, and mental impairment. With spinal anesthesia, a shot is given in the lower back to make patients numb below the waist. Sedation is then used so patients sleep through the surgery - this is often referred to as twilight sleep. Most patients who have spinal anesthesia have no memory of their time in the operating room.
How much pain am I going to have after surgery and how long will it last?
This varies for every patient. Understandably, the most common reason people delay having hip replacement surgery is fear of post-operative pain. Although there is no way to eliminate the pain completely, many things can be done both during and after surgery to minimize pain and speed recovery. First of all, the anterior approach I now offer is generally less painful than traditional surgical approaches because no muscle is cut during the operation. After surgery the nurses can give intravenous pain medicine every 2 hours, as needed. Almost all patients are switched over to oral painkillers after the first night. Most patients take pain medicine for 2-4 weeks after surgery.
Will I have to limit my weight bearing?
Most patients are allowed to put full weight on the their hip immediately after surgery.
How long do I have to use a walker or crutches?
At first, a walker or crutches provides needed support, but as your strength improves and pain decreases you can switch to using a cane and eventually wean off support completely. Most people start weaning off of the walker or crutches after a couple of weeks, some even sooner. Remember that it’s better to walk smoothly with a cane than to limp around without one - walking with a limp can cause pain in your back or other joints.
How long will I be in the hospital?
Most patients will return home 2-3 days after surgery. Patients who are recovering slowly or don’t have much help at home may benefit from a short stay in rehab facility before returning back home. If you need to go to “rehab,” you will be given several choices and arrangements will be made by the social worker in the hospital.
How long does it take to recover from surgery?
Recovery time varies almost as much as people do. The patients who make the quickest recovery are generally those who are in the best overall health prior to surgery, but most people are back to normal daily activities within 3 months. Discomfort, strength, balance and flexibility all continue to improve for 12 months. Surprisingly, there are patients whose pain at the time of discharge from the hospital is already less than it was prior to the surgery.
How much Physical Therapy (PT) will I need?
The need for PT also varies a lot. All patients get PT in the hospital twice a day. After discharge I’ve found that most patients do very well exercising on their own and don’t need formal PT. Of course, care is always individualized based on needs.
How much walking can/should I do when I get home?
The best answer is “as tolerated.” That means gradually increase your activities. Trial and error will tell you how much activity is too much. If you have “overdone it,” then you may experience increased pain and swelling in your leg. Just take it easy for a day or two and then try again at a less intense level. Remember that the healing process takes months, not weeks!
What should I look out for when I return home after surgery?
Do not hesitate to call our office or your primary care physician if you have any health concerns. These are a few particular things to always look out for:
- Signs of Infection: You or a family member should check the incision every day for signs of infection. While it can be normal for the area around the incision and staples to be a little pink and even a little warm, it should not be red or hot. If there is ever redness that seems to be spreading you need to contact our office immediately or go to the Methodist Hospital Emergency Department. Fever and/or increasing pain in the hip can also be signs of infection and need prompt medical evaluation.
- Blood clot (DVT) in a leg vein can cause the leg to swell and become more painful. Everyone’s leg has some swelling after surgery, but if the amount of swelling suddenly increases and especially if the swelling doesn’t improve after elevating the leg, then you should call our office or go to the Emergency Department. A pulmonary embolism can cause chest pain, shortness of breath, and rapid heart rate and requires immediate attention.
- Constipation: Pain medicines (narcotics) can cause constipation. It helps to eat a high fiber diet and consider taking an over-the-counter stool softener (Colace) daily. If needed, consider also using a laxative such as Milk of Magnesia or Dulcolax and contact your primary care physician for further treatment as needed.
When can I stop wearing my TED hose?
Compression stockings (TED hose) help decrease swelling in the leg and reduce the risk of blood clots. I prefer that patients wear them on the operative leg for at least 2 weeks following surgery. Feel free to remove them while in bed each night and then replace them in the morning.
When can I stop taking the blood thinner?
The blood thinner is usually stopped 2-4 weeks after surgery. If you were on daily aspirin, it should be restarted when you first get home from the hospital.
When can I drive again?
There is no fixed amount of time that driving is prohibited. In general, when your driving leg has good strength and control and you are no longer taking pain medicine such as Hydrocodone (Norco), or Oxycodone (Percocet), then it should be okay to drive.
When can I go back to work?
It depends on what kind of work you do. People with desk jobs and flexible schedules can try to go back to work after a few weeks. People with jobs requiring prolonged standing and full eight-hour days, however, may need to wait for 2-3 months before returning to work.
Do I have to restrict my movement after surgery?
Your therapist will let you know if there are any restrictions. One of the benefits of the anterior approach for hip replacement is that the hip is generally more stable and less likely to dislocate compared to traditional approaches. Therefore, patients who have had a routine anterior approach hip replacement will NOT have any restrictions placed on their movement.
Since every person’s surgery is unique, there are times when temporary restrictions are needed after surgery. Not every person can have an anterior approach hip replacement and sometimes other issues can arise that require restrictions. The Physical Therapists at Methodist Hospital will teach whatever restrictions may be needed prior to discharge. Some patients will be asked to follow hip dislocation precautions, some will need to limit the amount of weight put on the operative leg and some will be asked to limit lifting the leg to the side (abduction).
Are there any travel restrictions?
It is best not to take any long trips for three months after surgery. While not an absolute requirement, this advice is given because the risk of blood clots remains higher than normal for about 3 months after hip replacement, and prolonged sitting in a car or plane can add to this risk.
When can I shower or bathe?
The initial surgical dressing is usually replaced two days after the surgery by a special waterproof dressing. With this new dressing you can shower right away. This dressing is designed to be left in place for one week and then it can be removed. At that point, most patients no longer need any dressing. You should, however, avoid taking baths or swimming until given the okay - usually 3 weeks after surgery.
When can I sleep on my side?
You can sleep on either your operative or non-operative hip whenever you feel comfortable doing so. It may be difficult to sleep on your stomach because it can be challenging to get into and out of that position.
When can I resume sexual activity?
Whenever you would like, unless you were given any restrictions after surgery
Will I be able to play sports and exercise again?
Regular exercise is encouraged. However, people with joint replacements should avoid high-impact types of exercise and sports such as running or basketball. The goal of hip replacement is to decrease or eliminate pain so that you can remain active. How much activity is too much? No one knows the exact answer to that question. Golf and doubles tennis can usually be resumed 3 months after surgery. I recommend no lifting or carrying more than 50 pounds.
Will I need to return for any follow-up after my recovery is complete?
Yes. X-rays can pick up signs of wear or loosening long before you feel any discomfort and therefore should be checked regularly. The frequency of follow-up will be based on your activity level and it can vary from visits once a year to once every five years.
Will I set off metal detectors at the airport?
Most people with hip replacements do set off the metal detector. Simply tell the TSA agent before you pass through the metal detector that you have had a hip replacement. If you set off the metal detector, the agent is required to pull you aside and check you individually. Unfortunately, there is no TSA-approved ID card available.
Is it true I’ll have to take antibiotics before any dental work?
Yes. For a minimum of two years after a total joint replacement it is recommended that you take a single dose of oral antibiotic before any procedure that could introduce bacteria into your blood stream. This includes dental work, colonoscopy, cystoscopy (bladder ‘scope), and some other procedures. This is to prevent “seeding” of your artificial joint by bacteria, resulting in an infection. I prefer that my patients continue this practice indefinitely.
